Premium USA-Made Research Compounds
Browse lab-tested peptides, research liquids, capsules and more.
For laboratory and research use only. Not for human consumption.
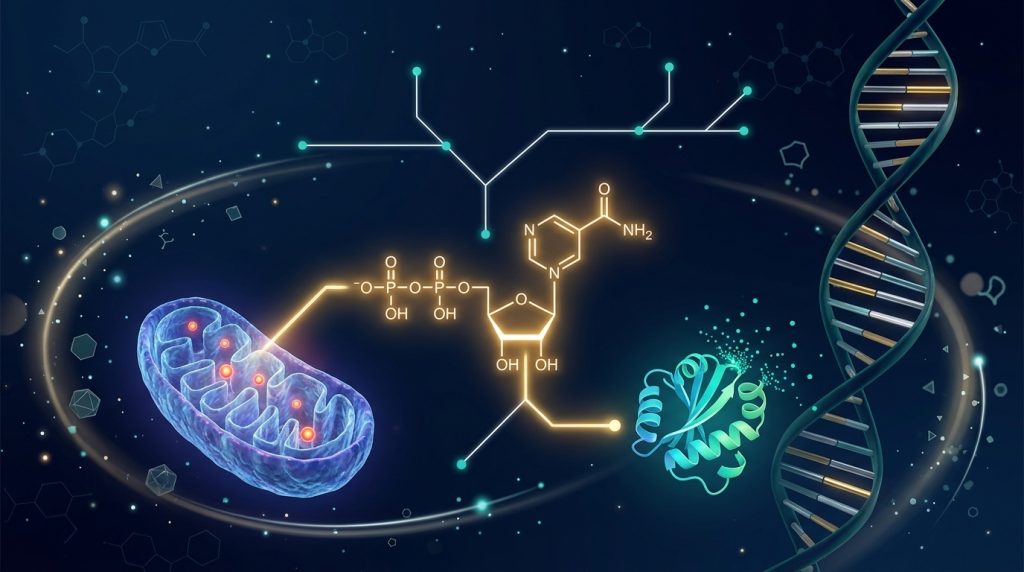
Here’s a problem that frustrated endocrine researchers for decades: native growth hormone-releasing hormone breaks down in minutes. Literally minutes. You inject it, enzymes chew it apart, and it’s gone before it can do much of anything useful. That’s why Theratechnologies Inc. in Montreal started tinkering with the molecule in the first place — and what they came up with was tesamorelin, a 44-amino acid GHRH analogue with one clever tweak that changes everything.
That tweak? A trans-3-hexenoic acid group bolted onto the N-terminal tyrosine. It sounds minor. It isn’t. That single lipophilic modification makes the compound resist the very enzymes that destroy native GHRH, and it tightens binding at the pituitary receptor. The result is one of the most studied growth hormone secretagogues in the research literature — with Phase 3 data, controlled trials, and head-to-head comparisons against compounds like sermorelin and CJC-1295.
Looking for Premium Research Compounds?
What Is Tesamorelin? Chemical Identity & Structure
Tesamorelin is a GHRH receptor agonist — a synthetic peptide that copies what your body’s own growth hormone-releasing hormone does. It carries the full 44-amino acid sequence of human GHRH (1-44). Same building blocks. One critical addition at the front end.
| Property | Value |
|---|---|
| Compound Name | Tesamorelin (TH9507) |
| Brand Name | Egrifta / Egrifta SV |
| CAS Number | 218949-48-5 |
| Molecular Formula | C221H366N72O67S |
| Molecular Weight | 5,135.86 Da |
| Amino Acid Length | 44 residues |
| Classification | GHRH receptor agonist |
| N-Terminal Modification | trans-3-Hexenoic acid |
| PubChem CID | 146681838 |
| Storage | 2–8°C (lyophilized powder) |
So why does that N-terminal modification matter so much? Two reasons. First, the trans-3-hexenoic acid group shields the peptide from DPP-IV and other aminopeptidases — the enzymes that shred native GHRH within minutes. Second, it actually improves how tightly the compound grabs onto receptors on pituitary somatotroph cells. Without the modification, endogenous GHRH (1-44) has a circulating half-life of maybe 5 to 7 minutes. That’s it. Gone. (PMID: 16052083). Tesamorelin survives long enough to do real work.
Development History
The compound started life as TH9507 — lab code, no brand name, just a promising molecule in Theratechnologies’ pipeline. The goal was straightforward: build a GHRH analogue that doesn’t fall apart the second it enters the bloodstream.
They succeeded. After Phase 2 and Phase 3 trials looking at how tesamorelin affected visceral fat stores, the FDA approved it in November 2010 under the brand name Egrifta. That made it the first — and still only — GHRH analogue with FDA approval specifically for reducing excess abdominal adiposity. Since then, researchers have been pulling at new threads: liver fat, muscle composition, even cognitive function. The compound keeps showing up in new contexts.
Mechanism of Action: How Tesamorelin Triggers GH Release
Big picture: tesamorelin binds the GHRH receptor on your pituitary. Pituitary releases growth hormone. Done. But if you’re designing protocols around this compound, you need to know what’s happening under the hood — because the cascade matters.
Pituitary GHRH Receptor Binding
Inject it subcutaneously. Tesamorelin finds GHRH receptors on somatotroph cells sitting in the anterior pituitary and latches on. And here’s the kicker — that trans-3-hexenoic acid mod creates a tighter grip than native GHRH manages. Stronger binding. Stronger activation. More potent signaling right from the start (PMID: 16052083).
The Signaling Chain
Receptor engagement sets off a domino run:
- Gαs protein flips on — activating adenylyl cyclase
- cAMP floods in — adenylyl cyclase converts ATP to cyclic AMP, fast
- PKA fires up — all that cAMP wakes protein kinase A
- CREB gets tagged — phosphorylated, shipped to the nucleus
- GH genes switch on — CREB parks on the GH1 promoter and transcription cranks up
- GH dumps into blood — simultaneously, PKA cracks open calcium channels and pre-formed GH granules pour out via exocytosis
Now here’s the piece that separates tesamorelin from just sticking someone with recombinant growth hormone. It preserves pulsatile release. Your body’s natural rhythm. Somatostatin still pumps the brakes between pulses. Feedback loops stay wired. You don’t get a flat-line dump of exogenous hormone — you get the real pattern, the one your pituitary was designed to produce. If you’re studying physiological GH secretion, this is a critical distinction. Not a minor footnote. Critical.
The IGF-1 Handoff
GH is actually a middleman. The real metabolic work? That falls on IGF-1. Growth hormone reaches the liver and other tissues, and IGF-1 production ramps. Fat breakdown, tissue remodeling, body composition shifts — IGF-1 runs most of that show. Researchers use IGF-1 elevation as their proof-of-concept marker for tesamorelin activity (PMID: 18057338). If IGF-1 isn’t moving, the compound isn’t working. Simple as that.
Published Research Findings
This isn’t a compound with a handful of pilot studies and some hand-waving. Tesamorelin has randomized controlled trial data. Multiple trials. Here’s what they found.
Visceral Fat: The Big One
Falutz et al. pooled data from two multicenter, double-blind, placebo-controlled Phase 3 studies — 816 subjects, 26 weeks (PMID: 23015655). The numbers were clear:
- Tesamorelin groups: −15.2% visceral adipose tissue vs. baseline
- Placebo groups: +5.0% — they gained visceral fat
- Between-group difference: P<0.001
- Trunk fat dropped too
A 20-point swing between drug and placebo. In an earlier Phase 2 trial with 61 subjects over 12 weeks (PMID: 16052083), the higher-concentration group hit −16% VAT reduction vs. −5% with placebo. Different study, same story.
Liver Fat: This Is Where It Gets Really Interesting
Stanley et al. ran a 12-month randomized controlled study with 60 subjects who had excess abdominal adiposity (PMID: 24823457). What they found caught a lot of attention:
- Tesamorelin cut hepatic fat fraction by 37% relative to baseline
- Placebo group? Their liver fat went up 27%
- Absolute drop: −3.7 percentage points tesamorelin vs. +1.7 placebo
- More subjects in the tesamorelin arm met criteria for hepatic steatosis resolution
Follow-up analyses showed that the liver fat reduction tracked with lower ALT levels and reduced hepatic inflammation markers. That’s pushed tesamorelin into NAFLD research — a field that’s been hunting for effective interventions for years.
Muscle Composition
This one snuck up on people. A secondary analysis from two randomized trials, published in Clinical Infectious Diseases (PMC6766405), used CT imaging on 341 subjects and found something nobody expected:
- Tesamorelin responders showed bigger increases in muscle density across four truncal muscle groups (1.56–4.86 Hounsfield units; all P<0.005)
- Both lean anterolateral/abdominal and rectus muscles improved (1.39 and 1.78 HU; P<0.005)
- All while visceral fat was going down
Losing visceral fat and improving muscle quality at the same time. That caught the attention of sarcopenia researchers pretty quickly.
Cognitive Function
This is newer and still developing. The GH-IGF-1 axis plays roles in neuroplasticity, hippocampal function, and neuroprotection — we’ve known that for a while. A Phase 2 trial (NCT02572323) started testing tesamorelin’s effects on cognitive performance in aging subjects with documented impairment. Full results are still being analyzed, but the rationale isn’t a stretch: IGF-1 promotes neurogenesis and synaptic plasticity in exactly the brain regions responsible for memory formation.
Metabolic Parameters Beyond Body Comp
Fat and muscle aren’t the whole picture. Published data also shows:
- Triglycerides: Improved trig levels and trig-to-HDL ratios in tesamorelin groups (PMID: 23015655)
- Adiponectin: Went up. That’s an adipokine linked to better insulin sensitivity — a good sign
- C-reactive protein: Some studies saw hsCRP drop, suggesting the visceral fat reduction carries anti-inflammatory effects along with it
- Glucose: Doesn’t appear to worsen fasting glucose or HbA1c in most populations, though the GH-IGF-1 axis does interact with insulin signaling in ways that researchers need to keep on their radar (PMID: 18057338)
Pharmacokinetics: What Researchers Need to Know
Numbers first:
| Parameter | Value |
|---|---|
| Route | Subcutaneous injection |
| Bioavailability (SC) | ~4% (typical for large peptides) |
| Tmax | ~0.15 hours (~9 minutes) |
| Half-life | 26 min (tesamorelin); 38 min (GHRH 1-44 fragment) |
| Peak GH Response | 15–60 min post-injection |
| IGF-1 Elevation | Sustained over weeks of administration |
| Metabolism | Proteolytic cleavage to GHRH(1-44) and smaller fragments |
| Protein Binding | Not fully characterized; lipophilic N-terminal modification may enhance tissue distribution |
Four percent bioavailability. That sounds terrible — and for a small molecule, it would be. But it’s normal for large peptides. The thing to wrap your head around: tesamorelin itself is gone from plasma in about 26 minutes. But the GH pulse it triggers lasts 2 to 4 hours. And the IGF-1 bump builds up over weeks of repeated dosing. So the compound disappears fast, but its biological footprint doesn’t. That disconnect between pharmacokinetics and pharmacodynamics is something researchers absolutely must account for in protocol design (PMID: 36356032).
Tesamorelin vs. Other GHRH Analogues
If you’re running GH secretagogue experiments, you’ve probably looked at sermorelin, CJC-1295, and tesamorelin side by side. Here’s how they stack up:
| Property | Tesamorelin | Sermorelin | CJC-1295 (no DAC) | CJC-1295 (with DAC) |
|---|---|---|---|---|
| Amino Acids | 44 | 29 | 29 (modified) | 29 (modified) |
| GHRH Sequence | Full GHRH(1-44) | GHRH(1-29) | Modified GHRH(1-29) | Modified GHRH(1-29) |
| Key Modification | trans-3-hexenoic acid (N-term) | None (truncated native) | 4 amino acid substitutions | 4 substitutions + DAC |
| Half-life | ~26 min | ~10–20 min | ~30 min | ~8 days |
| GH Release Pattern | Pulsatile | Pulsatile | Pulsatile | Sustained/blunted pulsatility |
| DPP-IV Resistance | Enhanced (N-terminal mod) | Minimal | High (amino acid subs) | High |
| IGF-1 Elevation | Significant, sustained | Moderate | Moderate | Prolonged |
| Visceral Fat Data | Extensive Phase 3 data | Limited | Limited | Limited |
| Published Trials | Multiple Phase 2/3 RCTs | Moderate | Limited | Limited |
Against Sermorelin
Sermorelin is GHRH chopped to 29 amino acids. Still works — the truncated fragment keeps full receptor activity. Pulsatile release? Check. But there’s no N-terminal shield. DPP-IV enzymes tear it apart. You’re looking at a 10-to-20-minute half-life, weaker GH bumps, and a pretty thin published record on visceral fat compared to tesamorelin’s Phase 3 dataset.
Against CJC-1295
Different philosophy here. CJC-1295 without DAC — Mod GRF 1-29 if you prefer the other name — swaps out four amino acids at positions 2, 8, 15, and 27. Those substitutions block DPP-IV from cutting the chain. Half-life: about 30 minutes. Comparable to tesamorelin. Keeps pulsatile release intact. And it stacks well with ghrelin agonists like ipamorelin — researchers like that combination for synergistic GH output.
Then there’s CJC-1295 with DAC. Totally different beast. The Drug Affinity Complex grabs serum albumin and hangs on, pushing the half-life to around 8 days. Eight days from one injection. Sounds ideal until you realize it might flatten the natural GH pulse pattern. If your experiments need physiological rhythm, that trade-off could be a deal-breaker.
Combo Approaches
Why pick one when you can push from both sides? Plenty of researchers pair GHRH agonists with ghrelin receptor agonists for synergistic GH release. Two different receptor systems, one combined output. The CJC-1295/Ipamorelin blend is the classic pairing. Ipamorelin earned its reputation by selectively boosting GH without dragging cortisol or prolactin along for the ride — cleaner than the older options like hexarelin, GHRP-2, or GHRP-6.
Safety Profile & Research Considerations
The pooled Phase 3 analysis (PMID: 23015655) gives a reasonably clear safety picture across hundreds of subjects:
- Injection site reactions: Most common finding. Redness, itching, induration at the injection point — typical peptide stuff
- IGF-1 went up: Consistently. But it dropped back to baseline when administration stopped. Reversible
- Glucose: Some subgroups saw small fasting glucose increases, but HbA1c changes weren’t statistically significant in most analyses
- Fluid retention: Some peripheral edema and joint discomfort — expected with GH-mediated effects
- Liver enzymes: ALT levels didn’t differ between tesamorelin and placebo groups across studies. No acute liver injury cases reported (PMID: 18057338)
One thing researchers need to know: the benefits reverse when you stop. Visceral fat reaccumulates after discontinuation. That’s a real consideration for long-term study designs — and for interpreting what “sustained effect” actually means with this compound.
Regulatory Status
FDA approved November 2010. Brand name: Egrifta (later reformulated as Egrifta SV in a single-vial format). It’s the only FDA-approved GHRH analogue specifically indicated for reducing excess abdominal fat in a defined regulatory context. Ongoing research extends into hepatic steatosis, cognitive function, and diabetic retinopathy — well beyond the original approval scope.
For lab research, tesamorelin is available as lyophilized powder at ≥98% purity, confirmed by third-party HPLC and mass spectrometry.
Product Specifications
| Specification | Details |
|---|---|
| Product | Tesamorelin 10mg |
| Form | Lyophilized powder |
| Purity | ≥98% (HPLC verified) |
| Third-Party Testing | Mass spectrometry + HPLC |
| Storage | 2–8°C, protect from light |
| CAS Number | 218949-48-5 |
Related compounds for GH axis research: Sermorelin 2mg, CJC-1295 (Mod GRF 1-29) 2mg, CJC-1295 with DAC 2mg, CJC-1295/Ipamorelin Blend, and Ipamorelin 2mg.
Where Tesamorelin Research Is Heading
The compound isn’t sitting still. Multiple angles are being explored right now:
NAFLD is the big one. Stanley’s liver fat work blew a door open, and now researchers want to know if those results hold across broader populations. Fatty liver disease affects tens of millions of people and treatment options are limited. Tesamorelin’s 37% relative reduction in hepatic fat is hard to ignore.
Cognition is the wild card. A Phase 2 trial (NCT02572323) is asking whether GH-IGF-1 axis activation can actually improve memory in aging subjects with cognitive impairment. It’s not a random bet — IGF-1 literally drives hippocampal neurogenesis. But we’ll need the data before getting too excited.
Sarcopenia crept in through the back door. Nobody expected those CT muscle density findings, but now there’s real interest in whether tesamorelin can fight age-related muscle decline while also trimming visceral fat.
Diabetic retinopathy and combination protocols — pairing tesamorelin with ghrelin agonists for synergistic metabolic effects — round out the active research landscape.
Conclusion
Tesamorelin is the GHRH analogue with the receipts. Phase 3 data showing 15.2% visceral fat reduction. A 37% relative cut in liver fat. Muscle density improvements that weren’t even the primary endpoint. And a mechanism that keeps pulsatile GH secretion intact instead of flooding the system with exogenous hormone.
Not many research peptides have this depth of controlled trial data behind them. For anyone studying GH axis modulation, body composition, or hepatic fat metabolism, it’s hard to skip past tesamorelin. Tesamorelin 10mg is available in high-purity lyophilized form for laboratory research.
References
- Falutz J, et al. Effects of tesamorelin on visceral fat and metabolic parameters. J Clin Endocrinol Metab. 2007. PMID: 16052083
- Falutz J, et al. Multicenter study of tesamorelin for visceral adiposity. J Acquir Immune Defic Syndr. 2008. PMID: 18057338
- Falutz J, Mamputu JC, Potvin D, et al. Pooled analysis of two Phase 3 trials with safety extension data. Clin Infect Dis. 2012;54:1642-51. PMID: 23015655
- Stanley TL, et al. Tesamorelin reduces hepatic fat in adults with excess abdominal adiposity. J Clin Endocrinol Metab. 2014. PMID: 24823457
- Adrian S, et al. Tesamorelin decreases muscle fat and increases muscle area. Clin Infect Dis. 2019. PMC6766405
- NCT02572323. Phase II Trial of Tesamorelin for Cognition. ClinicalTrials.gov.
For laboratory and research use only. Not for human consumption. This article is intended for educational and informational purposes for qualified researchers.
Continue Your Research
Explore our complete catalog of premium research compounds.