Premium USA-Made Research Compounds
Browse lab-tested peptides, research liquids, capsules and more.
CJC-1295 DAC vs CJC-1295 without DAC: research comparison of half-life, GH pulse patterns, IGF-1 elevation, and lab applications. (129 chars)
CJC-1295 DAC vs CJC-1295 Without DAC: Research Differences, Half-Life & Laboratory Applications
For research use only. Not intended for human consumption or any clinical application.
Same foundational sequence. Wildly different behavior. That’s the short version — but the short version misses almost everything that matters for study design.
Looking for Premium Research Compounds?
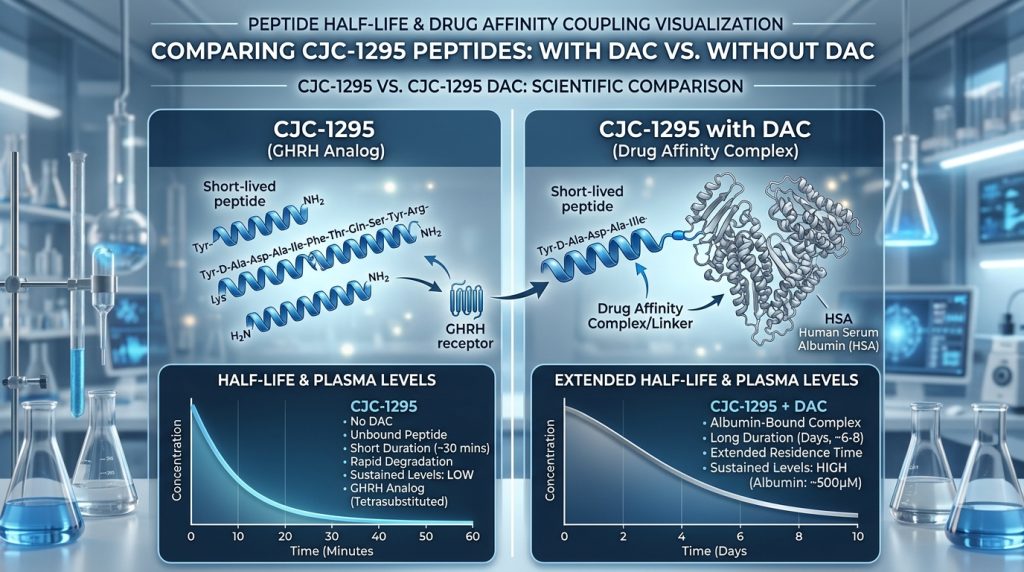
On paper, CJC-1295 DAC and CJC-1295 without DAC look like minor variants. In a narrow structural sense, they are. Both are synthetic analogs of growth hormone releasing hormone (GHRH). Both share the same 29-amino acid active region. What separates them is one molecular modification — the Drug Affinity Complex — that turns a peptide lasting roughly 30 minutes in circulation into one persisting for nearly a week. Six to eight days, specifically. Compare that to 30 minutes for Mod GRF 1-29. Same origin, wildly different behavior in circulation.
That gap isn’t cosmetic. It reshapes the entire research picture — GH secretion patterns, IGF-1 response kinetics, what experimental questions each compound can meaningfully address in an animal model, and frankly, which one will produce interpretable data in the first place.
What Is CJC-1295? The GHRH Analog Foundation
Here’s the thing about GHRH in its native form — it doesn’t survive long enough to study properly. Growth hormone releasing hormone is a 44-amino acid hypothalamic peptide that binds receptors on somatotroph cells in the anterior pituitary to trigger GH secretion. But dipeptidyl peptidase IV (DPP-IV) cleaves it rapidly. Serum half-life: 2–7 minutes in most animal models. Studying sustained GHRH signaling with the native peptide is essentially impossible under laboratory conditions.
So the modifications came in stages. GRF 1-29 preserved full receptor binding while dropping the C-terminal tail. Then four strategic amino acid substitutions — Ala at positions 2, 8, and 27; Gln at position 15 — produced Modified GRF 1-29, blocking DPP-IV cleavage and extending stability to roughly 30 minutes. CJC-1295 takes it further still, attaching the Drug Affinity Complex to that Mod GRF 1-29 backbone.
Worth flagging a terminology issue that causes real problems in the literature: “CJC-1295” gets applied loosely to both forms. That’s not just imprecise — it’s the kind of conflation that actively undermines study interpretation and reproducibility. These are genuinely different compounds. The distinction that gets overlooked most often is also, inconveniently, the most consequential one for experimental design.
The Drug Affinity Complex (DAC) Technology — How It Works
The DAC modification is, mechanistically speaking, quite elegant. A lysine residue is added to the C-terminus of Modified GRF 1-29. That lysine gets conjugated with maleimido propionic acid (MPA). The MPA group then forms a reactive thioether bond with a free cysteine-34 on serum albumin — the most abundant plasma protein in circulation.
Albumin binding — covalent in this case — is what makes it work.
Albumin carries a serum half-life of approximately 19 days in most mammalian systems. Compounds that successfully bind albumin essentially hitchhike on that stability, dramatically extending their own circulation time. For CJC-1295 DAC, the result is a plasma half-life of approximately 6–8 days in preclinical models. That’s not a single-study finding — it’s been confirmed across multiple published references, which is, frankly, a large part of why the DAC version gets used at all.
The binding is covalent and persistent. Not permanent — the molecule eventually dissociates and clears — but persistent enough to produce effects that play out over days rather than minutes. Critically, the GHRH receptor-binding region remains active even while albumin-bound. Published data supports continued bioactivity throughout the extended half-life window. Extended persistence and extended functional signaling. Both.
DAC technology was developed by ConjuChem as a generalized platform for extending short-lived peptide half-lives. The GHRH-DAC compound remains one of the most thoroughly studied applications of that platform.
Half-Life Comparison: CJC-1295 DAC vs CJC-1295 Without DAC
The half-life numbers are striking. Six to eight days. Compare that to 30 minutes for Mod GRF 1-29. Same origin, wildly different behavior in circulation.
Here’s what that means laid out plainly:
| Property | CJC-1295 Without DAC (Mod GRF 1-29) | CJC-1295 With DAC | |||| | Plasma half-life | ~30 minutes | ~6–8 days | | Albumin binding | No | Yes (covalent, via MPA-lysine) | | GH secretion pattern | Acute pulses, rapid clearance | Sustained “GH bleed,” attenuated pulsatility | | Dosing frequency in research | High (to achieve desired GH pulses) | Low (once weekly or less in most models) | | IGF-1 elevation duration | Transient per administration | Sustained elevation over days | | Research utility | Pulsatile GH studies, GHRP co-administration | Sustained GH axis activation, body composition models |
The Teichman et al. (2006) study published in the Journal of Clinical Endocrinology & Metabolism is the foundational reference for CJC-1295 DAC half-life data — preclinical work subsequently replicated and extended those findings in both rodent and primate models. For the without-DAC form, 30 minutes is an average; actual clearance varies by species. Even so, that’s a massive improvement over native GHRH’s 2–7 minute window, which is exactly why Mod GRF 1-29 became a standard tool for acute GH pulse research in the first place.
GH Pulse Patterns — Blunted Waves vs. Preserved Pulsatility
This is where the two compounds diverge most meaningfully. And it deserves more than a passing mention in study design discussions.
In normal physiology, GH is released in pulses. The hypothalamus fires GHRH in burst-like patterns, somatostatin provides inhibitory counterbalance, and what emerges from the pituitary is episodic secretion — not flat, continuous output. Published research has linked GH pulse amplitude and frequency to downstream effects on body composition, metabolism, and tissue signaling. The pulses aren’t just a delivery mechanism. They’re part of the signal itself. That’s not a trivial distinction.
CJC-1295 without DAC allows relatively precise modulation of those GH pulse patterns in animal models. Administered at defined intervals, it produces distinct GH secretion peaks followed by return to baseline — mimicking the pulsatile architecture of natural GHRH signaling. Particularly useful when researchers want to observe downstream events from a controlled GH pulse. Especially when combining with ghrelin mimetics like ipamorelin, which works through a completely separate receptor pathway.
CJC-1295 DAC produces a fundamentally different pattern. The GH bleed — that sustained, low-level release pattern — is actually one of the more debated aspects of DAC research. Persistent GHRH receptor stimulation over days creates continuous low-amplitude GH secretion without pulsatile architecture. Total GH output can be substantial, but it arrives as a trickle rather than episodic surges. Studies interested in cumulative IGF-1 response or long-duration body composition changes may find the DAC version appropriate. Studies investigating pulsatile secretion dynamics? The DAC version would actively interfere with the signal they’re trying to measure.
Research Findings: CJC-1295 DAC in Animal Models
Let’s be specific about what the animal data actually shows.
The most cited work comes from Jetté et al. (2005), published in Endocrinology (146(6):2734–2740). Male rats, single and multiple administrations, GH and IGF-1 tracked throughout. It remains a solid reference point, though the broader literature is thinner than many would expect for a compound that’s been around this long — more extensively characterized pharmacokinetically than mechanistically, and that gap is exactly where independent research has been filling in.
From that foundational work and subsequent animal studies, several findings hold up across replications:
A single administration produced measurable GH elevation persisting for several days in rodent models — consistent with the extended half-life profile. Multiple-dose protocols produced further accumulation rather than plateau. Serum IGF-1 rose significantly and remained elevated throughout the multi-day window; increases of 2–3× baseline were documented in some rodent studies at higher research concentrations, which is actually quite striking against native GHRH comparators.
Chronic administration produced body weight increases, with some studies noting preferential lean mass accretion relative to fat mass. Liver, spleen, and other GH-responsive tissues showed changes consistent with sustained somatotropic signaling in long-term protocols — directly relevant for preclinical safety characterization.
On tachyphylaxis: some data suggests prolonged GHRH receptor stimulation can lead to receptor desensitization. Whether and how quickly this develops under DAC’s long-acting profile remains an active area of investigation, at least based on what the rodent models currently show.
Research Findings: CJC-1295 Without DAC (Modified GRF 1-29)
Mod GRF 1-29 has a broader footprint in the preclinical literature — partly because it more closely tracks natural GHRH behavior, partly because its use in combination protocols is so widespread.
In practice, what this means for study design is substantial. In rodent and primate models, Mod GRF 1-29 reliably produces acute serum GH spikes within 15–30 minutes — mirroring native GHRH-triggered pulses with consistent, reproducible amplitudes. That consistency makes it a solid positive control for GH axis research, which is, frankly, underappreciated as a methodological asset.
Receptor selectivity matters here too. Mod GRF 1-29 binds specifically to GHRH receptors on somatotrophs — it doesn’t engage the ghrelin/GHS-R1a pathway, and that’s not a trivial distinction when attributing observed effects to a specific molecular pathway rather than a compound mix.
Because the compound clears quickly, GH levels return toward baseline between administrations. Cleaner experimental windows, better temporal resolution. Several preclinical studies have used Mod GRF 1-29 in models of GH deficiency, obesity, and metabolic dysfunction specifically because its ability to restore pulsatile GH patterns lets researchers investigate pulse restoration versus continuous GH elevation — a question the DAC form simply cannot address.
Researchers who’ve worked with this compound in aged animal models tend to report consistent findings: in older rodent subjects where endogenous GHRH output naturally declines, Mod GRF 1-29 administration documents restoration of GH pulse amplitude. Those results hold up well across aging model replication attempts.
IGF-1 Elevation and Downstream Effects in Research
Both forms elevate IGF-1. The kinetics differ substantially — and that matters more than it sometimes gets credit for.
IGF-1 is produced primarily in the liver in response to GH signaling. In research settings, it serves as a surrogate marker for sustained GH axis activation — measuring acute GH pulses requires frequent sampling, whereas IGF-1 integrates GH activity over time. Useful property. But it also means the measurement collapses temporal information that the two CJC-1295 forms encode very differently. Is that a problem? In some research contexts, yes — particularly when the dynamics of GH secretion are the actual variable of interest.
With CJC-1295 DAC, IGF-1 elevation is pronounced and sustained. Rodent findings have documented it remaining elevated for 9–11 days following a single administration in certain protocols. That persistence is why the DAC version has found utility in body composition and metabolic research — the sustained IGF-1 signal drives downstream effects on protein synthesis, fat metabolism, and tissue growth signaling that don’t accumulate in short-window experiments.
With Mod GRF 1-29, each administration produces a transient GH spike and corresponding short-duration IGF-1 response. Cumulative effect depends on administration frequency, which can be an advantage when researchers want to titrate response or observe dose-frequency relationships that the DAC form’s built-in persistence makes impossible to isolate.
Downstream — mTOR signaling, protein synthesis rates in muscle tissue, lipolysis in adipose models, bone formation markers. The DAC form suits studies where these cascades need days to play out. The without-DAC form suits studies where temporal precision is the whole point. Practically speaking, that distinction should come before any other study design consideration.
Ipamorelin Combination Studies — Synergistic Research Context
One of the most active areas of CJC-1295 research involves co-administration with ipamorelin. Here’s why it works the way it does.
Ipamorelin is a selective GH secretagogue — a ghrelin receptor (GHS-R1a) agonist. Where GHRH analogs stimulate GHRH receptors on somatotrophs to increase GH release, ipamorelin simultaneously suppresses somatostatin through a different receptor pathway. The two mechanisms are complementary, not redundant. One presses the accelerator. The other releases the brake. That’s not a metaphor — it’s the actual dual-pathway mechanism behind the synergistic effect.
Animal research has consistently documented substantially larger GH pulses when GHRH analogs and GH secretagogues are co-administered. The without-DAC form + ipamorelin combination is particularly well-suited to pulsatile GH release research: both compounds can be timed to produce synchronized pulses with clear onset and offset. Published animal studies have documented amplified GH peaks, measurable IGF-1 increases, and downstream body composition changes across multiple replication attempts.
The DAC + ipamorelin combination tells a different story. The DAC form maintains constant background GHRH receptor stimulation, while ipamorelin administrations layer additional pulses on top of that basal GH bleed. Relevant to endocrine aging and GH-deficient animal research — but the secretion profile it generates is genuinely different from the no-DAC combination. Specifying which CJC-1295 form is used isn’t just good scientific practice. It’s the minimum requirement for reproducibility.
Choosing Between Forms: Laboratory Design Considerations
So which form actually matters for research? It depends entirely on what the study is trying to answer. Here’s a practical framework built from published research applications rather than abstractions.
Choose CJC-1295 Without DAC (Mod GRF 1-29) when:
- The objective involves pulsatile GH release — amplitude, frequency, or temporal dynamics
- Co-administration with ipamorelin or other GHRPs is planned and synergistic pulse amplification is the goal
- Temporal resolution matters — clean GH peaks and troughs with minimal inter-dose carryover
- Studying GH pulse restoration in aged or GH-deficient animal models
- Shorter experimental windows where frequent administration is feasible and precision is the priority
Choose CJC-1295 With DAC when:
- The objective is sustained GH axis activation over days or weeks
- Long-term body composition studies where cumulative GH and IGF-1 elevation is the independent variable
- IGF-1 needs to remain consistently elevated throughout the observation window
- Reduced administration frequency matters operationally — in animal models where frequent injections create confounding stress responses, for example
- Anti-aging endocrine models where tonic GH axis stimulation is the experimental condition
One critical point that gets missed: the DAC form is poorly suited for research asking questions about pulsatile versus tonic GH release. Published reviews have explicitly flagged this mismatch. Using the DAC form in that context isn’t just suboptimal — it produces data that answers a different question than the one the study was designed to investigate. That’s the kind of mistake that doesn’t surface until after the work is already done.
Stability, Storage & Reconstitution in Research Settings
Practically speaking, the storage question matters more than it might seem — especially for a compound like CJC-1295 DAC where the reactive MPA group introduces handling variables that the without-DAC form doesn’t share.
Both forms are supplied in lyophilized (freeze-dried) powder form, and the baseline handling protocols are largely consistent between them.
Lyophilized storage: −20°C in sealed vials away from light and moisture for long-term storage — stability holds for 24 months or more. Working stock: 4°C for material used within 1–3 months. Avoid repeated freeze-thaw cycling; the structure degrades with each cycle.
Reconstitution: Bacteriostatic water is standard. Sterile water works, but shortens post-reconstitution stability. Add solvent slowly down the vial wall rather than directly onto the lyophilized cake, then swirl gently — vortexing causes peptide aggregation and is one of the more common handling errors with this compound class. Post-reconstitution, store at 4°C; published guidance supports 4–6 weeks of refrigerated stability for bacteriostatic water preparations.
DAC-specific handling note: The maleimide group is sensitive to hydrolysis under non-ideal conditions — compromised DAC functionality defeats the purpose of using the compound at all. Reconstituted CJC-1295 DAC should be used promptly; avoid extreme pH or temperatures outside the recommended range. Third-party COA documentation confirming purity ≥98% by HPLC is the baseline verification step before research use.
Conclusion
CJC-1295 DAC and CJC-1295 without DAC are not interchangeable research tools. They don’t answer the same questions — and treating them as interchangeable produces exactly the kind of ambiguity the preclinical literature has struggled with since both forms entered circulation under the same name.
The DAC modification transforms a short-acting GHRH pulse generator into a sustained somatotropic axis activator. Plasma half-life of 6–8 days, covalent albumin binding through the MPA-lysine conjugate, extended functional signaling throughout. That window makes it the right tool for body composition research, long-duration IGF-1 elevation studies, and metabolic models that simply aren’t feasible with short-acting compounds.
The without-DAC form — Mod GRF 1-29 — preserves pulsatile research capability. Its 30-minute half-life closely tracks natural GHRH pulse kinetics, making it the right tool when temporal GH secretion dynamics are the focus. Combined with ipamorelin, it produces some of the most robust synergistic GH pulse data in the preclinical literature.
Both compounds have meaningful preclinical datasets behind them. The choice between them is a study design decision — one that shapes everything downstream. Understanding the mechanistic and pharmacokinetic differences between these two forms isn’t background knowledge. It’s where clean, reproducible, interpretable research actually starts.
All information in this article is intended for research and educational purposes only. CJC-1295 (DAC and without DAC) is for laboratory use in research settings. Not for human consumption or clinical application.
Continue Your Research
Explore our complete catalog of premium research compounds.